
Comments: Aneurysm of The Pulmonary Artery
Samba Niang*
Department of pneumology of the university hospital center, St. Louis, Senegal
Pulmonary tuberculosis is associated with many complications or sequelae that can lead to hemoptysis. More than a third of patients will have an episode of hemoptysis during the natural history of their tuberculosis.
In about 80% of the cases, a bronchial artery or another systemic artery is at the origin of the bleeding but in the remaining 20%, a pulmonary arterial origin is found1.
In tuberculosis, two different forms of pulmonary arterial pseudoaneurysm can be schematically distinguished:
In acute tuberculosis, the extension of caseous necrosis, to a pulmonary artery destroys the three tunics, and a pseudoaneurysm, a source of hemoptysis, of classically moderate abundance. The mechanism is the same as for any necrotizing lung disease.
The Rasmussen aneurysm develops, on the contrary, in contact with a chronic tuberculous cavern, at a distance from the acute phase. Its description has been the subject of numerous publications2,3. Rémy et al.4 emphasized this potentially lethal form of the false erosive aneurysm, highlighting their lack of knowledge, the concept of "sentinel" hemoptysis, a possible prelude to fatal hemoptysis, and, above all, the possibilities of interventional angiography5.
In this observation, hemoptysis was probably related to an acquired aneurysm, possibly from an infectious cause, given the history of pulmonary tuberculosis: Rasmussen's aneurysm. But in the absence of data on pulmonary and right ventricular arterial pressures, we can not formally eliminate an idiopathic congenital aneurysm from the pulmonary arteries or secondary to a systemic disease such as Behçet's inflammatory arteritis.
The major risk of aneurysm of the pulmonary artery is represented by rupture (one-third of all-cause patients) or dissection6.
Smalcelj et al. described a 33-year progressive dissected giant aneurysm that reached 15.7 cm at the trunk of the pulmonary artery, complicating rupture one year later7.
Yaméogo et al. 8 described a similar aneurysm of the trunk of the pulmonary artery (74mm) and its divisional branches (28mm to the right and 36mm to the left) associated with mitral stenosis. Reported cases of aneurysmal pulmonary artery disease are associated with either pulmonary valve stenosis or PAH9,10. However, in our, no cardiac exploration (Doppler echo or right heart catheterization) had been performed to formally eliminate right valvular stenosis or associated pulmonary arterial hypertension.
Hemoptysis resulting from Rasmussen aneurysms results from an intimal fissure in its most vulnerable zone and bronchopulmonary flooding (figure). They may temporarily dry up during local thrombosis or cranial obstruction of the drainage bronchus, but recurrence is common.
Currently, the diagnosis is based on the angio-TDM which overcomes the false negatives of the angiography. The appearance is that of a sacciform aneurysm rather tending to a distal branch (figure) than to a proximal trunk.
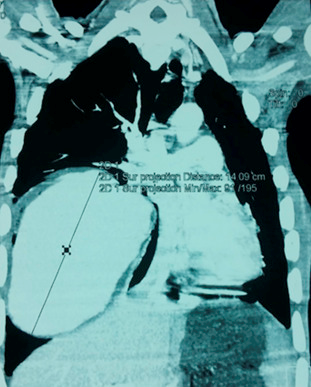
Figure : Chest angio-CT, mediastinal window. Giant aneurysm 4.09 cm from the trunk of the right pulmonary artery. Note a control peripheral halo of fissure of the aneurysm.
The size varies from 5 mm to 3 cm, but giant aneurysms have been described. The angiography is from the beginning therapeutic, it is usefully guided by the tomodensitometric reconstructions: seat and size of the neck. The resulting embolization gesture must meet the requirements of prudence and precision.
Surgery remains the treatment of choice in the absence of contraindication, to prevent rupture or dissection.
Auerbach et al. published in 1939 an autopsy series of 1114 patients with pulmonary tuberculosis with cavitary lesions and found 45 cases of pulmonary arterial aneurysm (4%), 38 of which were responsible for fatal haemoptysis11. Similarly, Plessinger et al. published in 1956 a series of 56 cases of Rasmüssen's aneurysm. In 47 (87%) cases, massive pulmonary arterial hemorrhage was responsible for death12.
Although rare, this pathology remains responsible for significant lethality due to the severity of the associated hemoptysis and requires special care.
In our case, the technical plateau being limited locally, the angiography could not be performed, a cataclysmic haemoptysis had occurred at the time of evacuation with rapid death of the patient.
Conclusion
Aneurysms of the pulmonary artery represent a rare pathology of multifactorial etiology dominated by infectious causes and Behçet's disease. Their symptomatology is not specific and their diagnosis is based on thoracic angiography.
The evolution can be silent contrasting with the often large size of the pulmonary arteries. The major risk is represented by rupture or dissection of the aneurysm.
References
- Sanyika C, Corr P, Royston D, et al. Pulmonary angiography and embolization for severe hemoptysis due to cavitary pulmonary tuberculosis. Cardiovasc Intervent Radiol. 1999; 22(6): 457-60.
- Auerbach O. Pathology and pathogenesis of pulmonary arterial aneurysm in tuberculous cavities. Am Rev Tuberc. 1939; 39: 99- 115.
- Plessinger VA, Jolly PN. Rasmussen’s aneurysms and fatal hemorrhage in pulmonary tuberculosis. Am Rev Respir Dis. 1949; 60: 589- 603.
- Rémy J, Smith M, Lemaitre L, et al. Treatment of massive hemoptysis by occlusion of a Rasmussen aneurysm. Am J Roentgenol. 1980; 135: 605- 606.
- Patankar T, Prasad S, Deshmukh H. Fatal hemoptysis caused by ruptured giant Rasmussen’s aneurysm. Am J Roentgenol. 2000; 174: 262- 263.
- Durak D, Eren B, Turkmen N, et al. Pulmonary artery aneurysm rupture Bratisl Lek Listy. 2008; 109: 582-583.
- Smalcelj A, Brida V, Samarzija M, et al. Giant, dissecting, high-pressure pulmonary artery aneurysm: case report of a 1-year natural course Tex Heart Inst J. 2005; 32: 589-594.
- Yaméogo NV, Ndiaye MB, Diao M, et al. Dilatation anévrismale de l’artère pulmonaire et de ses branches sur sténose mitrale à propos d’un cas Ann Cardiol Angeiol. 2011; 10.1016/j.ancard.2010.12.020
- Shankarappa RK, Moorthy N, Chandrasekaran N, et al. Giant pulmonary artery aneurysm secondary to primary pulmonary hypertension Tex Heart Inst J. 2010; 37: 244-245.
- Ibn Elhadj Z, Keskes H, Kammoun I, et al. Anévrisme post-sténotique du tronc de l’artère pulmonaire chez un sujet de 70ans J Mal Vasc. 2011; 36: 399-400.
- Auerbach O. Pathology and pathogenesis of pulmonary arterial aneurysm in tuberculous cavities. Am Rev Tuberc. 1939; 39: 99-115.
- Plessinger VA, Jolly PN. Rasmussen’s aneurysm and fatal hemorrhage in pulmonary tuberculosis. Am Rev Tuberc. 1949; 60: 589-603.