
Commentary: Efficacy of antifibrotic drugs, nintedanib and pirfenidone, in treatment of progressive pulmonary fibrosis in both IPF and non-IPF
James Patrick Finnerty
Department of Respiratory Medicine, Countess of Chester Hospital NHS Trust, Liverpool Road, Chester, UK
Introduction
Idiopathic pulmonary fibrosis (IPF) is a specific form of chronic fibrosing interstitial lung disease associated with a pattern of Usual Interstitial Pneumonia (UIP) based on CT appearances or histology. Two drugs with anti-fibrotic effects have been licensed in the UK in the treatment of IPF: pirfenidone and nintedanib1,2. In the UK, use of these drugs was therefore initially restricted to UIP, as determined by local and regional multidisciplinary teams, and those patients whose condition did not meet the National Institute for Health and Care Excellence (NICE) criteria were ineligible to receive anti-fibrotic therapy. A meta-analysis and systematic review from myself and co-workers published last year reviewed the existing and growing evidence for the use of these anti-fibrotic drugs both in IPF and in patients with progressive disease in conditions that can not be classified as UIP, either because they are not readily classifiable at all, or because they fall into another clearly classified group, such as non-specific interstitial pneumonitis (NSIP) or hypersensitivity pneumonitis (HP)3. This commentary reviews that meta-analysis and its implications.
There were two underlying assumptions made in performing this meta-analysis. The first was that the published data suggested a similar efficacy between pirfenidone and nintedanib, at least as far as protecting against decline in forced vital capacity (FVC), in trials in patients with IPF: it was thus reasonable to group the two drugs together as anti-fibrotic therapy. The second assumption was that most if not all progressive non-IPF interstitial lung disease has lung fibrosis as the common final pathway, and that anti-fibrotic therapy may have just as much efficacy in reducing the rate of fibrosis and arresting decline in FVC in these non-IPF cases as in IPF.
Review of Meta-analysis
Our searches were restricted to published randomised controlled trials of either pirfenidone or nintedanib in the treatment of either IPF or non-IPF progressive interstitial lung disease. We restricted our data extraction on outcomes to all-cause mortality and changes in FVC. Changes in FVC were the primary outcome. FVC changes were expressed in a variety of ways, so the pooled FVC outcomes were expressed as a standardized effect size (Cohen’s d). All-cause mortality was a secondary outcome, reported in some studies (Table 1): we chose all-cause mortality as the most robust mortality measure rather than respiratory mortality which involves judgements that might vary from trial to trial. We did not publish extracted data on questionnaires on health status given the incompleteness of the data and variety of questionnaires used.
Eleven papers covering thirteen studies were included4-14 (Table 1). FVC data was extracted from all of these. Eleven had data on all-cause mortality: this was pooled for the two INPULSIS trials and the two CAPACITY trials, reducing the number of separate trials analysed for mortality to nine. Four of the studies were trials in patients with non-IPF, covering unclassifiable ILD, HP, NSIP, and ILD associated with a variety of connective tissue diseases.
Table 1: Summary of Included Studies
|
Studies |
Medication |
Disease |
N in study |
All-cause Mortality available |
|
Richeldi et al. TOMORROW Trial 2011 |
Nintedanib |
IPF |
167 |
Yes |
|
Richeldi et al. INPULSIS trial 1 2014 |
Nintedanib |
IPF |
513 |
Yes |
|
Richeldi et al. INPULSIS trial 2 2014 |
Nintedanib |
IPF |
548 |
Yes |
|
Flaherty et al. INBUILD trial 2019 |
Nintedanib |
Non-IPF |
412 |
Yes |
|
Distler et al. N Engl J Med 2019 |
Nintedanib |
Non-IPF |
576 |
Yes |
|
Azuma et al. 2005 |
Pirfenidone |
IPF |
109 |
No |
|
Taniguchi et al. 2010 |
Pirfenidone |
IPF |
212 |
No |
|
Noble et al. CAPACITY trial NCT 00287729 2011 |
Pirfenidone |
IPF |
348 |
Yes |
|
Noble et al. CAPACITY trial NCT 00287716 2011 |
Pirfenidone |
IPF |
344 |
Yes |
|
Huang et al. 2015 |
Pirfenidone |
IPF |
76 |
Yes |
|
King et al. ASCEND trial 2014 |
Pirfenidone |
IPF |
555 |
Yes |
|
Maher et al. 2020 |
Pirfenidone |
Non-IPF |
237 |
Yes |
|
Behr et al. 2021 |
Pirfenidone |
Non-IPF |
67 |
Yes |
The results for standardized changes in FVC showed an overall mean effect size of -0.306 (SE 0.033), p<0.001. We calculated a prediction interval for the distribution of true effect sizes assuming heterogeneity: the interval was between -0.18 to -0.43, indicating that regardless of drug used or condition treated, one would expect a useful effect size. In fact, we could not show a significant difference between pirfenidone and nintedanib (effect sizes -0.266 and -0.340 respectively). Nor was there a significant difference in anti-fibrotic efficacy between pooled data in IPF and non-IPF (effect sizes -0.305 and -0.307 respectively). To put this into perspective, the standardised change is the difference between active and placebo groups expressed as a proportion of the standard deviation in the underlying rate of change in FVC. As an example, in the cohort study by Nasser et al. of non-IPF FVC decline, the annual rate of FVC decline was -136 ml, with a standard deviation of 328 ml15. An effect size of -0.306 would give an expected annual rate of decline in the treatment group of -36 ml.
An analysis of all-cause mortality was performed in 9 studies where data was available. Overall mean risk ratio was 0.701 in favour of antifibrotic therapy (CI 0.539 to 0.911): for IPF this equated to 0.637 (CI 0.469 to 0.866) whereas for non-IPF it was 0.908 (CI 0.547 to 1.508). An all-cause mortality benefit was therefore not demonstrated in the non-IPF group. This may have been due to shorter studies in non-IPF with pirfenidone compared with pirfenidone studies in IPF, or to the smaller numbers studied overall where all-cause mortality was available.
Conclusions
Efficacy of anti-fibrotic therapy was very similar as judged by changes in FVC in IPF compared with non-IPF. It is reasonable to conclude that there is significant efficacy in anti-fibrotic therapy across a wide range of non-IPF progressive lung disease as regards lung function. The data were insufficient to establish whether this also applied to mortality.
Since publication of this meta-analysis, NICE have issued further guidance on nintedanib16. Nintedanib is now recommended as an option for treating chronic progressive fibrosing interstitial lung diseases (PFâILD) in adults in addition to its recommendation in IPF. The data are insufficient to recommend pirfenidone for non-IPF disease, but our meta-analysis suggests that it may have efficacy, given that there is no statistically significant difference shown between the two anti-fibrotic agents when their effect is pooled over IPF and non-IPF.
Further data, currently available in abstract form, has recently become available on the role of pirfenidone in ILD associated with rheumatoid arthritis17. The TRAIL 1 trial recruited during the pandemic, which took its toll: with an initial target of 270 participants, 123 were randomized between a placebo group (n=60) and a pirfenidone group (n=63) with a 52-week follow-up period. The mean annual decline in FVC was 66 ml in the pirfenidone group and 146 ml in the placebo group (P<0.01). These data have been incorporated in a re-run of our meta-analysis on FVC changes, and the pooled results for pirfenidone and nintedanib are shown in Figure 1. The groups compared were IPF versus Non-IPF, and the pooled data for each group is shown as a diamond shape., with a further diamond for the combined data. The Q statistic for difference between the groups was small at 0.062, and not statistically significant (p=0.804). The standardized difference for the pooled IPF data was -0.305 (confidence interval -0.389 to -0.222) (p<0.001). The standardized difference for the pooled non-IPF data was -0.312 (confidence interval -0.437 to -0.209) (p<0.001). Essentially, the previous conclusions are unchanged.
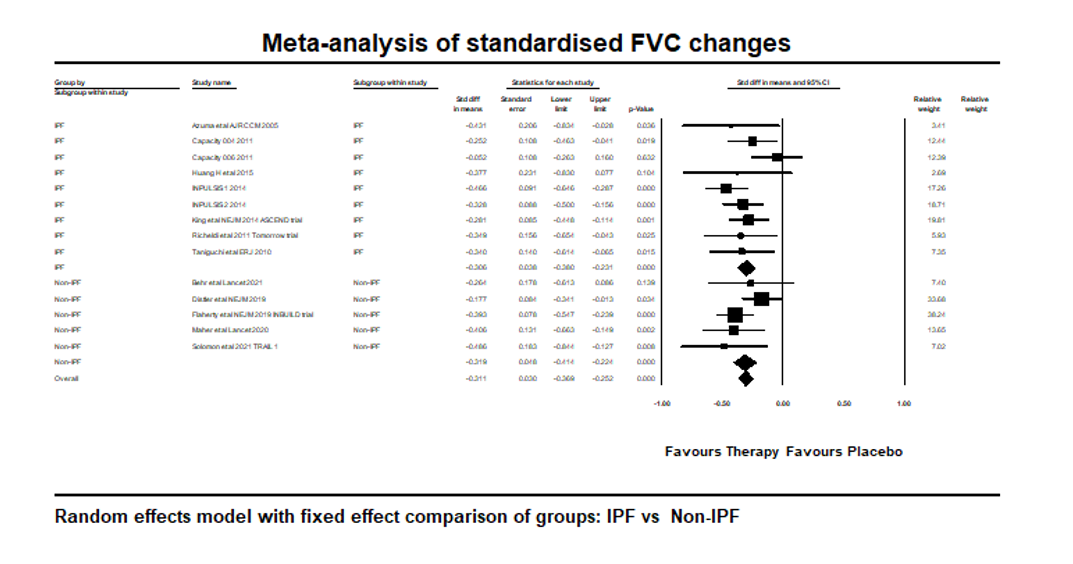
Figure 1:
References
- National Institute for Health and Care Excellence. Pirfenidone for treating idiopathic pulmonary fibrosis [London]; NICE: 2018 [reviewed 2022 March; cited 2022 March 11]. Technology appraisal guidance [TA504]. Available from: https://www.nice.org/guidance/ta504
- National Institute for Health and Care Excellence. Nintedanib for treating idiopathic pulmonary fibrosis [London]; NICE: 2016 [cited 2022 March 11]. Technology Appraisal guidance [TA379]. Available from: https://www.nice.org.uk/guidance/ta379
- Finnerty JP, Ponnuswamy A, Dutta P, et al. Efficacy of antifibrotic drugs, nintedanib and pirfenidone, in treatment of progressive pulmonary fibrosis in both idiopathic pulmonary fibrosis (IPF) and non-IPF: a systematic review and meta-analysis. BMC Pulmonary Medicine. 2021; 21(1): 411.
- Richeldi L, Du Bois RM, Raghu G, et al. Efficacy and Safety of Nintedanib in Idiopathic Pulmonary Fibrosis. New England Journal of Medicine. 2014; 370(22): 2071-82.
- Richeldi L, Costabel U, Selman M, et al. Efficacy of a Tyrosine Kinase Inhibitor in Idiopathic Pulmonary Fibrosis. New England Journal of Medicine. 2011; 365(12): 1079-87.
- Distler O, Highland KB, Gahlemann M, et al. Nintedanib for Systemic Sclerosis–Associated Interstitial Lung Disease. New England Journal of Medicine. 2019; 380(26): 2518-28.
- King TE, Bradford WZ, Castro-Bernardini S, et al. A Phase 3 Trial of Pirfenidone in Patients with Idiopathic Pulmonary Fibrosis. New England Journal of Medicine. 2014; 370(22): 2083-92.
- Flaherty KR, Wells AU, Cottin V, et al. Nintedanib in Progressive Fibrosing Interstitial Lung Diseases. New England Journal of Medicine. 2019; 381(18): 1718-27.
- Azuma A, Nukiwa T, Tsuboi E, et al. Double-blind, Placebo-controlled Trial of Pirfenidone in Patients with Idiopathic Pulmonary Fibrosis. American Journal of Respiratory and Critical Care Medicine. 2005; 171(9): 1040-7.
- Behr J, Prasse A, Kreuter M, et al. Pirfenidone in patients with progressive fibrotic interstitial lung diseases other than idiopathic pulmonary fibrosis (RELIEF): a double-blind, randomised, placebo-controlled, phase 2b trial. The Lancet Respiratory Medicine. 2021; 9(5): 476-86.
- Maher TM, Corte TJ, Fischer A, et al. Pirfenidone in patients with unclassifiable progressive fibrosing interstitial lung disease: a double-blind, randomised, placebo-controlled, phase 2 trial. The Lancet Respiratory Medicine. 2020; 8(2): 147-57.
- Noble PW, Albera C, Bradford Williamson Z. Pirfenidone in patients with idiopathic pulmonary fibrosis (CAPACITY): two randomised trials. Lancet. 2011; 377: 1760-69.
- Taniguchi H, Ebina M, Kondoh Y, et al. Pirfenidone in idiopathic pulmonary fibrosis. European Respiratory Journal. 2010; 35(4): 821-9.
- Huang H, Dai HP, Kang J, et al. Double-Blind Randomized Trial of Pirfenidone in Chinese Idiopathic Pulmonary Fibrosis Patients. Medicine. 2015; 94(42): e1600.
- Nasser M, Larrieu S, Si-Mohamed S, et al. Progressive fibrosing interstitial lung disease: a clinical cohort (the PROGRESS study). European Respiratory Journal. 2021; 57(2): 2002718.
- National Institute for Health and Care Excellence. Nintedanib for treating progressive fibrosing interstitial lung diseases [London]; NICE: 2021 [cited 2022 March 11]. Technology Appraisal guidance {TA747]. Available from: https://www.nice.org.uk/guidance/ta747
- Solomon J, Woodhead F, Danoff S, et al. A randomised, double-blinded, placebo-controlled, phase 2 study of safety, tolerability and efficacy of Pirfenidone in patients with rheumatoid arthritis interstitial lung disease. Arthritis Rheumatol. 2021; 73: abstract L10.